
Assessment of Cephalometric Changes in a Class II Patient Treated with Twin Block : A Case Report - By Dr. Tamara Marouf
4 min read
Abstract
Myofunctional appliances are used to encourage mandibular development by forward repositioning the mandible in growing individuals with Class II malocclusions due to mandibular retrusion(Clark, W.J., 1988).The effects of the myofunctional appliances is mostly dento-alveolar with small skeletal effect and greatly dependent on the patient’s compliance(O’Brien et al., 2003).In this case report a 10-year old Pubertal female patient was treated with Twin Block appliance followed by Fixed orthodontic mechanotherapy with preadjusted edgewise (MBT- 022 X 028” slot) appliance to detail the occlusion. The Twin Block appliance is widely recognized as a patient-friendly option for managing Class II malocclusions in growing patients with mandibular retrognathia. It functions by posturing the lower jaw forward using inclined planes incorporated into the bite blocks. This forward positioning modifies the neuromuscular balance and encourages adaptive growth at the condyles, resulting in favourable mandibular development. (Clark, W.J., 1988) This paper presents a case report demonstrating the successful use of this appliance.
Diagnostic Summary
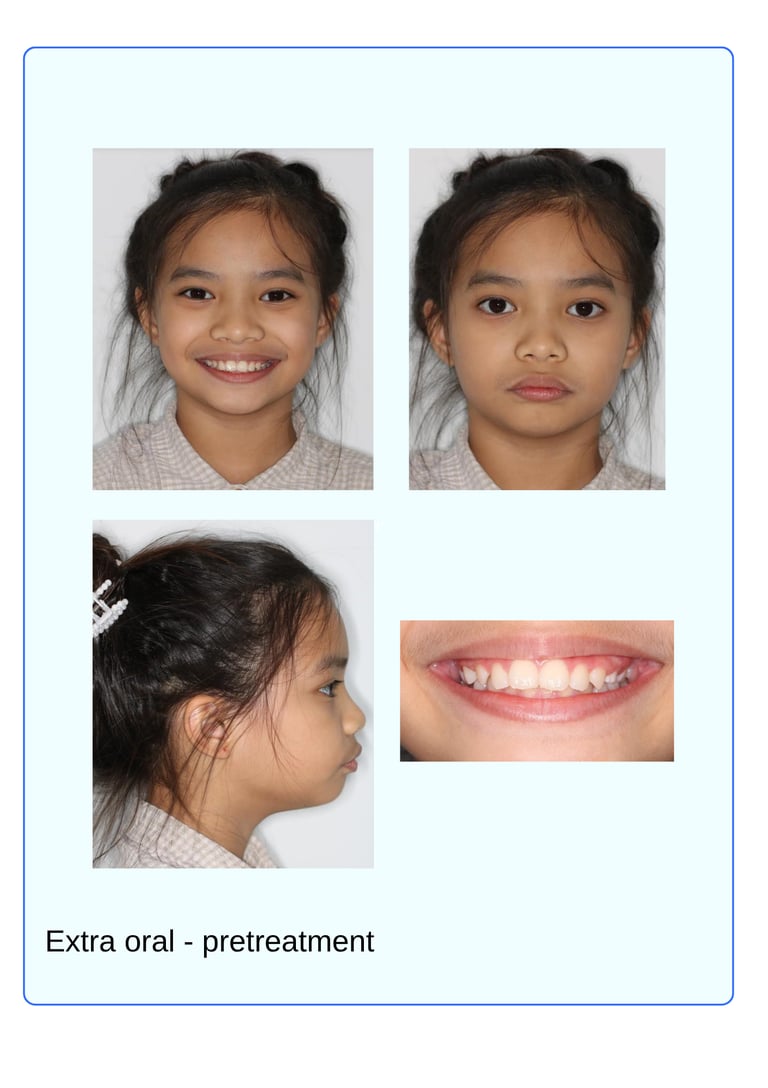
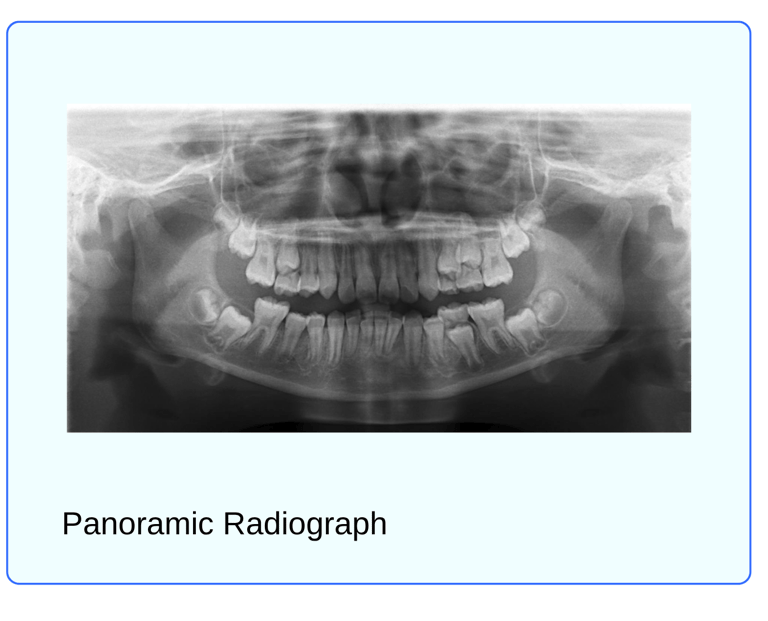
S.A is a 10 years old Asian female with a chief complaint “I don’t like how my teeth are sticking out and I get bullied at school” Clinically; she is class II division 1 Incisor relationship on skeletal class II sagittal basal relationship, with Horizontal growth pattern. This was complicated by a 6 mm overjet, class II (1/2 unit) canine relationship and molar relationship of class II on both sides, Mild crowding in the lower arch and a deep bite, with a convex profile, decreased lower anterior facial height potentially competent lips. IOTN Grade 3a Etiology of Malocclusion: Skeletal: Saggital class II with Mandibular Retrognathia, forward mandibular rotation Dental: Tooth size-Arch Length Discrepancy Soft tissue: Potentially competent lips and Mentalis hyperactivity, short upper lip, Adaptive tongue posturing
Treatment plan
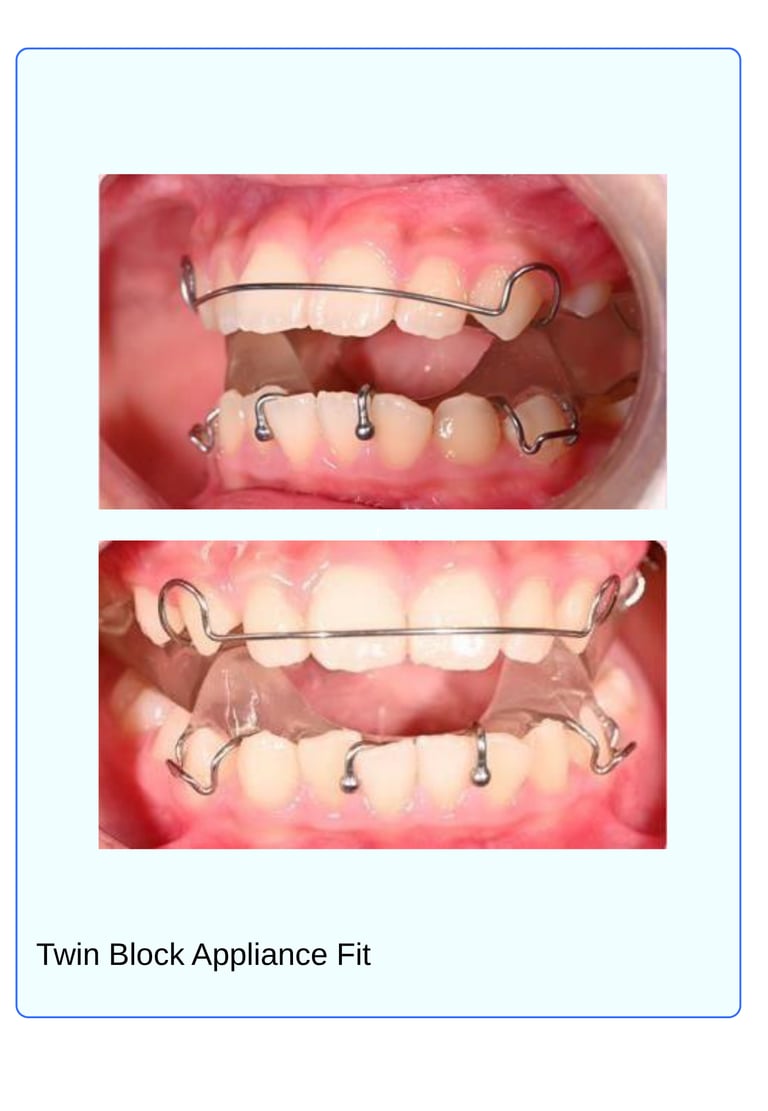
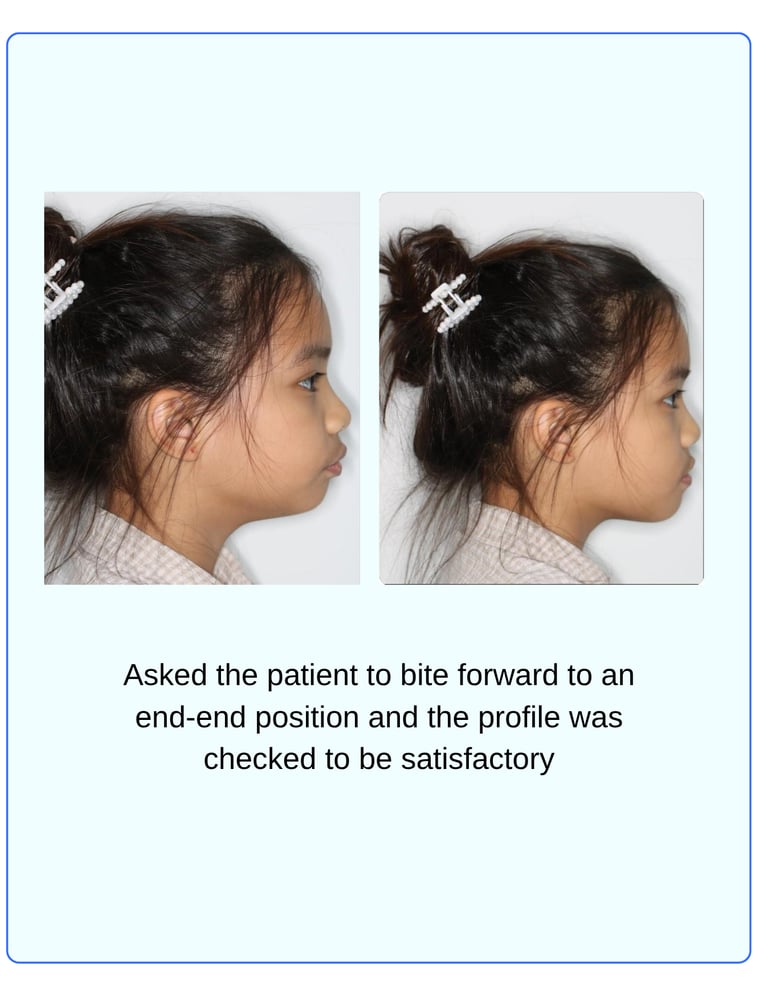
Treatment option: Two-Phase Treatment Non extraction with Functional Appliance: Growth modification treatment followed by Fixed pre-adjusted Appliance using 0.022" MBT brackets Active phase Twin block appliance full time wear for a period of 6-8 months(active tooth borne) • With progressively trimming the upper bite-block occlusodistally to allow the lower molars to erupt.
The lower block is trimmed over a period of 2 or 3 months to reduce the open bite in the premolar region. (This method of reducing overbite by controlled eruption of posterior teeth supported by occlusal biteblocks results in favorable changes in facial balance by increasing lower facial height) • Maintenance of the the corrected incisor relationship until the buccal segment occlusion is fully established
Support Phase: Transition to Nighttime wear of the Twin-block appliance until eruption of full permanent dentition Fixed Appliance Banding of upper molars and impression taken for anterior inclined Bite Plane(to assist in retaining the sagittal correction achieved with the Twin Block and to facilitate a smooth transition to fixed appliance therapy) Bonding of Upper and Lower Arch • Alignment and leveling using appropriate archwire sequence. • Assessment of the need for Class II elastics • Space closure • Finishing Retention:Hybrid using fixed retainer from 3-3 and Removable Essix with Anterior bite plane


Results
Skeletal:
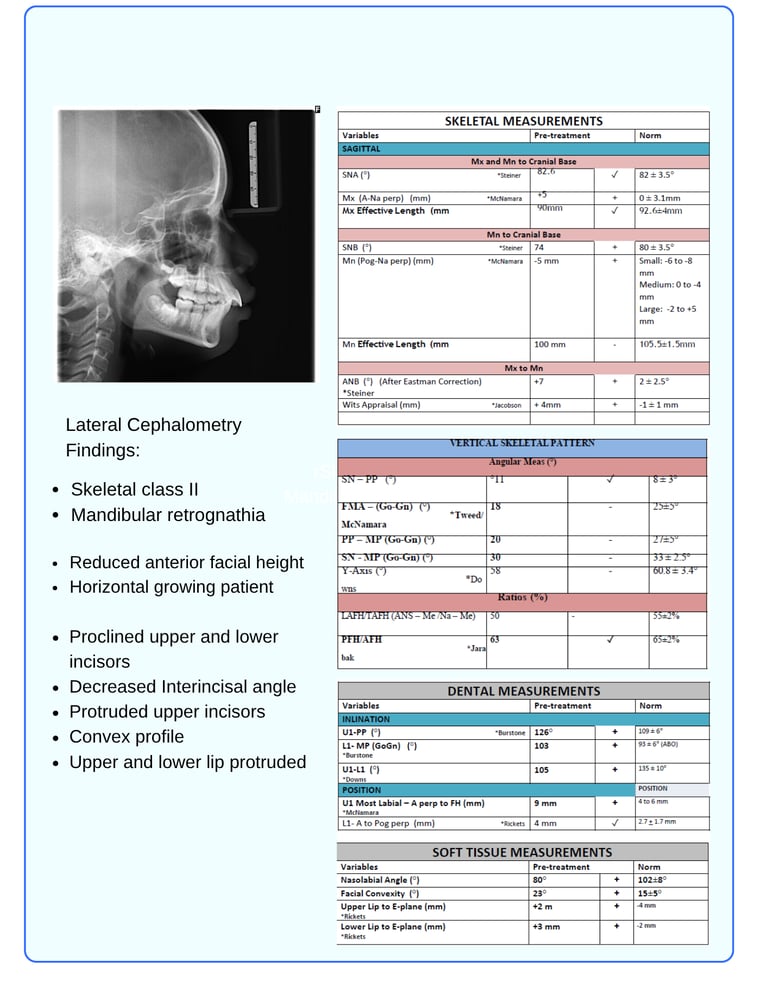
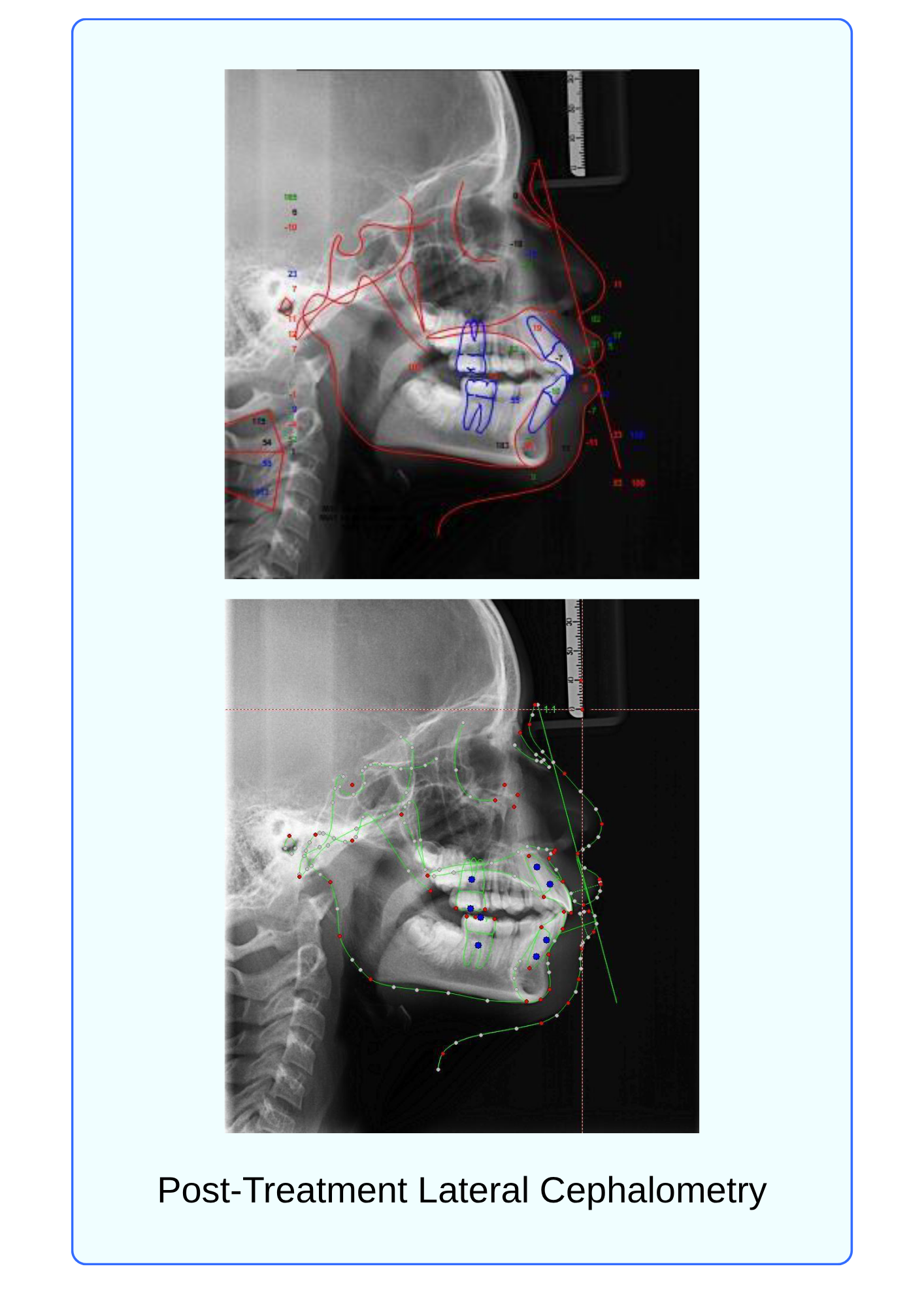
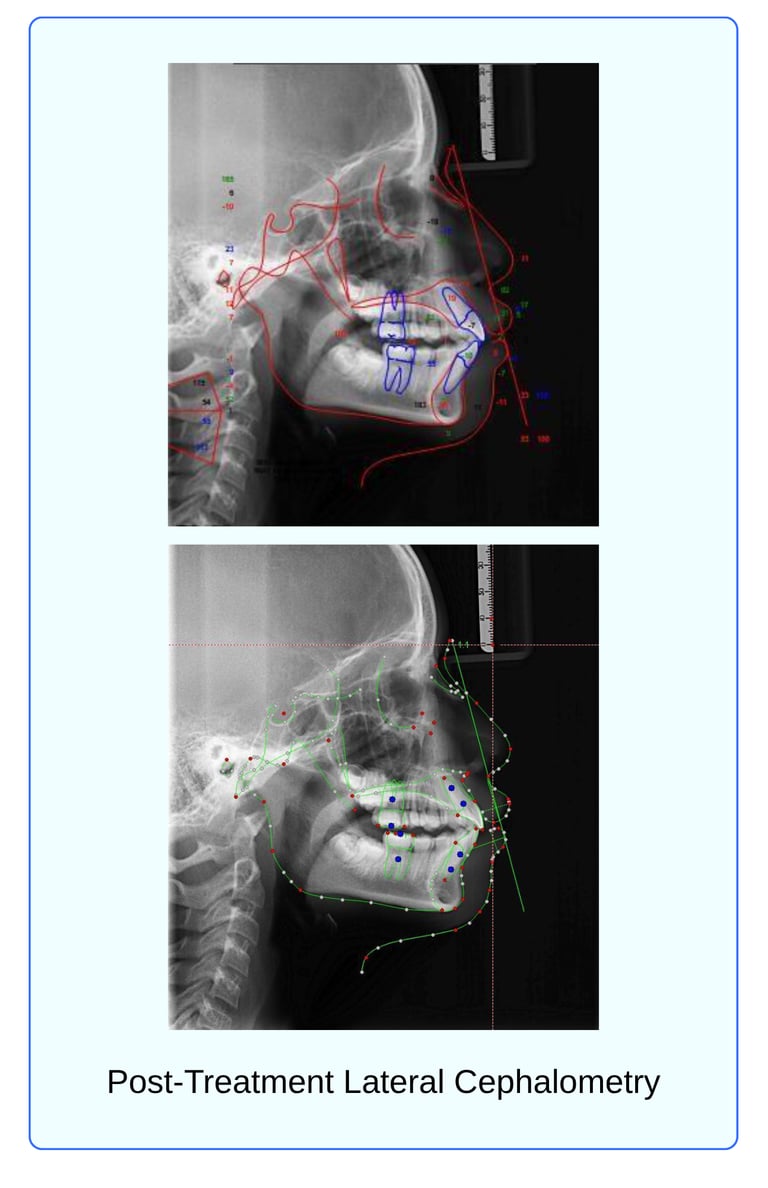
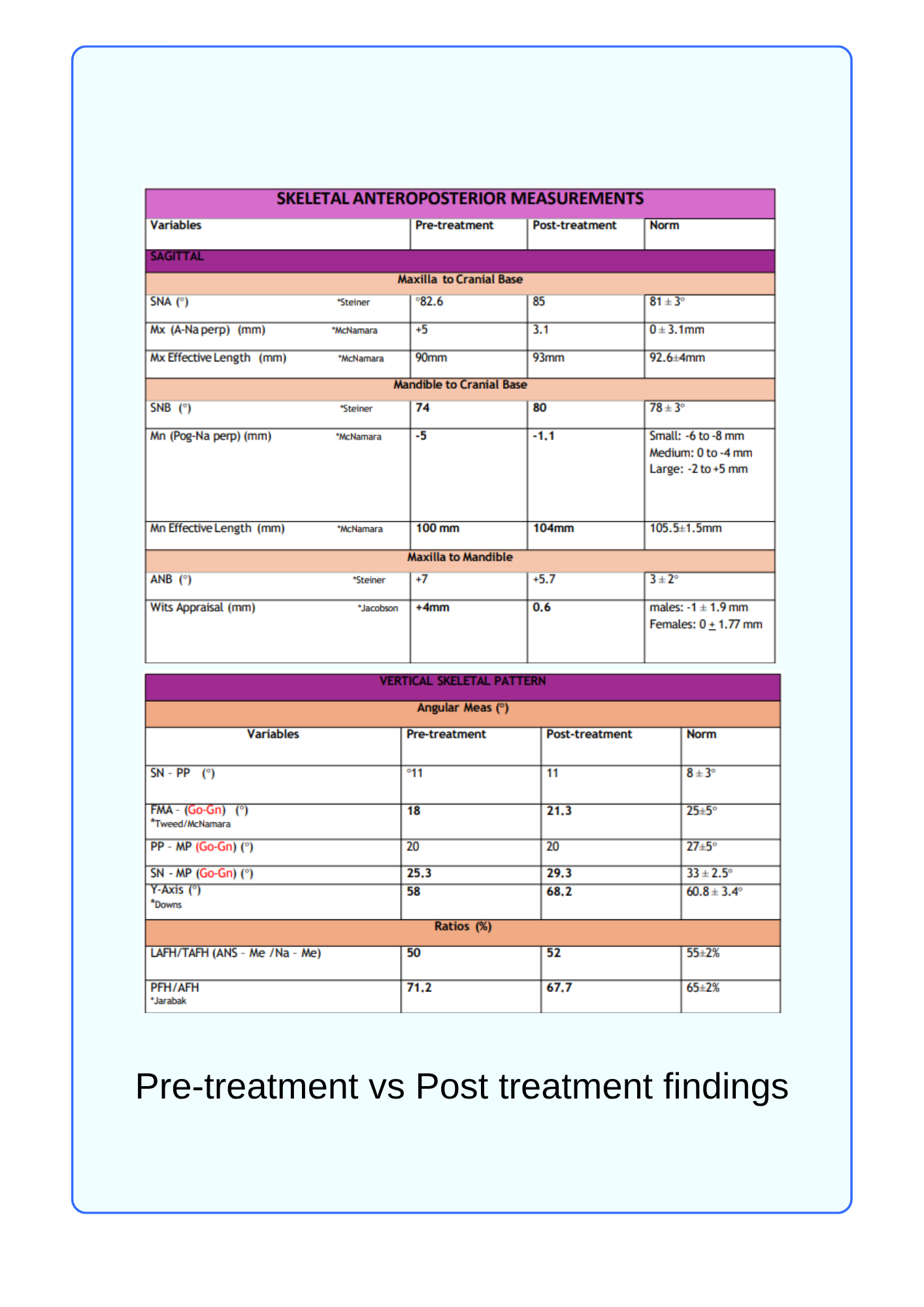
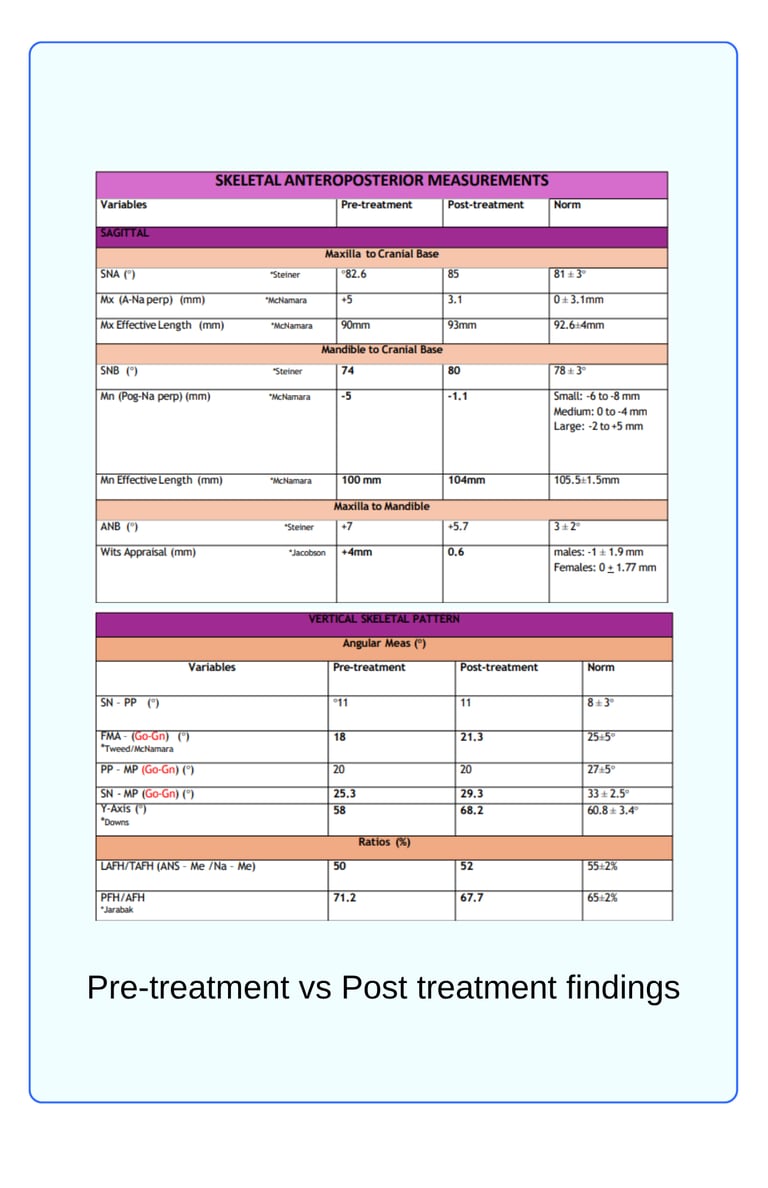
The cephalometric findings reveal significant skeletal, dental, and soft tissue improvements. Skeletally, the maxilla showed forward movement, with SNA increasing from 82.6° to 85° and A-Na perpendicular decreasing from +5 mm to 3.1 mm, indicating a shift toward normal.
Maxillary effective length increased from 90 mm to 93 mm. The mandible also advanced, as evidenced by an increase in SNB from 74° to 80°, and Pog-NA perpendicular improved from -5 mm to -1.1 mm. Mandibular effective length increased from 100 mm to 104 mm. ANB reduced from +7° to +5.7°, and Wits appraisal improved from +4 mm to 0.6 mm, reflecting a more balanced anteroposterior skeletal relationship.
In the vertical dimension, FMA increased from 18° to 21.3°, SN-MP from 25.3° to 29.3°, and Y-Axis from 58° to 68.2°, indicating vertical growth and mandibular clockwise rotation. LAFH/TAFH increased from 50% to 52%, while PFH/AFH decreased from 71.2% to 67.7%, suggesting a slight increase in lower anterior facial height.




Dental:
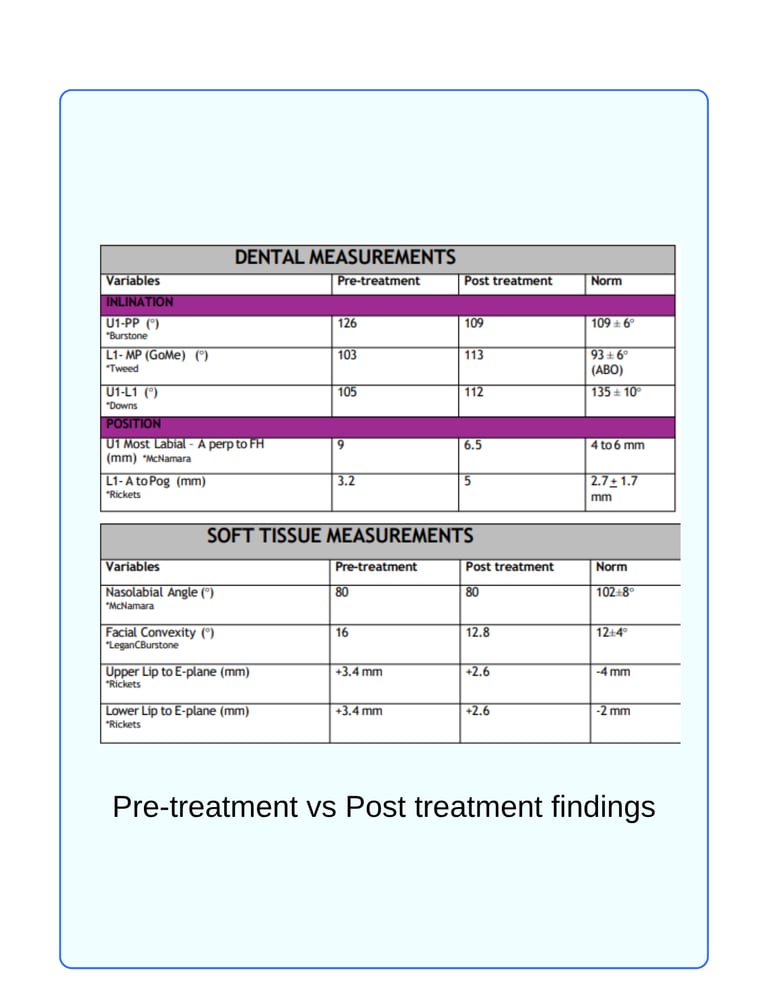
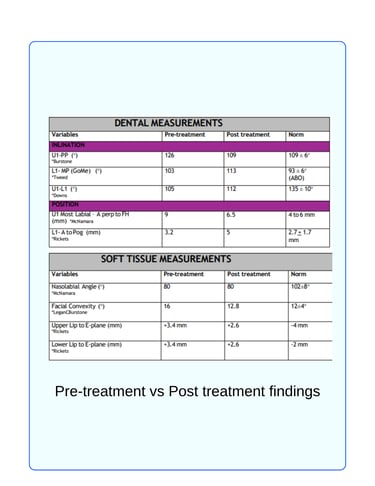
Dentally, upper incisor proclination decreased (U1–PP from 126° to 109°), while lower incisor proclination increased (L1–MP from 103° to 113°), resulting in a greater interincisal angle (U1–L1 from 105° to 112°). Upper incisor position improved relative to A-perpendicular (from 9 mm to 6.5 mm), and lower incisor position relative to A–Pog increased from 3.2 mm to 5 mm.
Soft Tissue:
Soft tissue analysis showed a more harmonious facial profile, with facial convexity decreasing from 16° to 12.8°. The nasolabial angle remained unchanged at 80°, still below the ideal range. Both upper and lower lips became less protrusive relative to the E-plane, reducing from +3.4 mm to +2.6 mm. Overall, the changes reflect significant skeletal advancement, dental compensation, and profile improvement
Conclusion
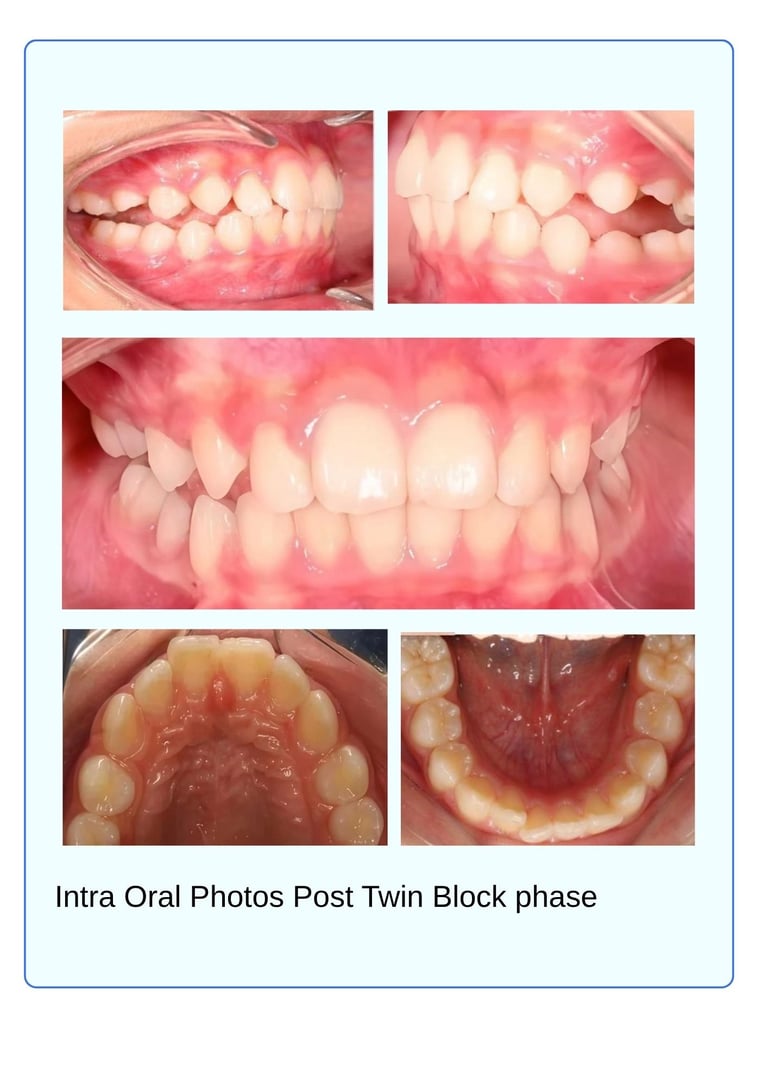
The twin block phase successfully achieved mandibular advancement and improved the skeletal anteroposterior relationship. Upon transitioning to the fixed appliance phase, these skeletal corrections were maintained while dental alignment and occlusion were refined. The case is now in the finishing stage, with proper overjet and overbite established. Both functional and esthetic objectives have been effectively achieved.
Dr. Tamara Marouf


